


 Sign Out
Sign Out



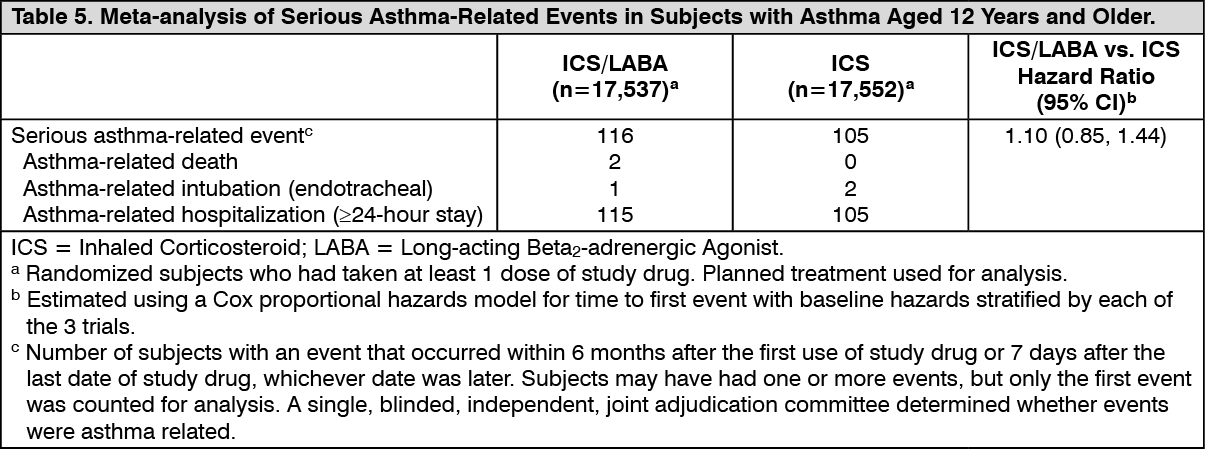
Serious Asthma-Related Events with Inhaled Corticosteroid/Long-acting Beta2-adrenergic Agonist Combination Products: Four (4) large, 26-week, randomized, double-blind, active-controlled clinical safety trials were conducted to evaluate the risk of serious asthma-related events when LABA were used in fixed-dose combination with ICS compared with ICS alone in subjects with asthma. Three (3) trials included adult and adolescent subjects aged 12 years and older: 1 trial compared budesonide/formoterol with budesonide, 1 trial compared fluticasone propionate/salmeterol with fluticasone propionate, and 1 trial compared mometasone furoate/formoterol with mometasone furoate. The fourth trial included pediatric subjects aged 4 to 11 years and compared fluticasone propionate/salmeterol with fluticasone propionate. No safety study was conducted with TRELEGY ELLIPTA. The primary safety endpoint for all 4 trials was serious asthma-related events (hospitalizations, intubations, death). A single, blinded, independent, joint adjudication committee determined whether events were asthma related.
The 3 adult and adolescent trials were designed to rule out a 2.0-fold increase in relative risk for ICS/LABA compared with ICS. Each individual trial met its pre-specified objective and demonstrated non-inferiority of ICS/LABA to ICS alone. A meta-analysis of the 3 adult and adolescent trials did not show a significant increase in risk of a serious asthma-related event with ICS/LABA fixed-dose combination compared with ICS alone. These trials were not designed to rule out all risk for serious asthma-related events with ICS/LABA compared with ICS. (See Table 5)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSalmeterol Multicenter Asthma Research Trial (SMART): A 28-week, placebo-controlled, U.S. trial that compared the safety of salmeterol with placebo, each added to usual asthma therapy, showed an increase in asthma-related deaths in subjects receiving salmeterol (13/13,176 in subjects treated with salmeterol versus 3/13,179 in subjects treated with placebo; relative risk: 4.37 [95% CI: 1.25, 15.34]). Use of background ICS was not required in SMART. The increased risk of asthma-related death is considered a class effect of LABA monotherapy.
Not for Acute Use: TRELEGY ELLIPTA should not be used for the relief of acute symptoms of COPD or asthma (i.e., as rescue therapy for the treatment of acute episodes of bronchospasm). Patients should be prescribed a rapid onset, short duration inhaled bronchodilator (e.g., salbutamol) to relieve acute symptoms such as shortness of breath, and advised to have this available for use at all times.
When beginning treatment with TRELEGY ELLIPTA, patients who have been taking a rapid onset, short duration, inhaled bronchodilator on a regular basis should be instructed to discontinue the regular use of these drugs and use them only for symptomatic relief if they develop acute symptoms while taking TRELEGY ELLIPTA.
Deterioration of Disease and Acute Episodes: TRELEGY ELLIPTA should not be initiated in patients with acutely deteriorating COPD or asthma which may be a life-threatening condition. The use of TRELEGY ELLIPTA in this setting has not been studied and is not considered appropriate.
COPD or asthma may deteriorate acutely over a period of hours or chronically over several days or longer. If TRELEGY ELLIPTA no longer controls symptoms of bronchoconstriction, the patient's inhaled, short-acting bronchodilator becomes less effective or the patient needs more inhalation of a short-acting bronchodilator than usual, these may be markers of deterioration of disease. In this setting, a re-evaluation of the patient and the treatment regimen should be undertaken at once.
Asthma-related adverse events and exacerbations may occur during treatment with TRELEGY ELLIPTA.
Patients should be advised to continue treatment and seek medical advice if symptoms remain uncontrolled or worsen after initiation of therapy with TRELEGY ELLIPTA.
Patients should not stop therapy with TRELEGY ELLIPTA without physician supervision since symptoms may recur after discontinuation.
Excessive use and use with other LABA and LAMA products: TRELEGY ELLIPTA should not be used more often or at higher doses than recommended.
TRELEGY ELLIPTA should not be administered concomitantly with other medicines containing a long-acting beta2-adrenergic agonist (e.g., salmeterol, formoterol fumarate, indacaterol, olodaterol), or a long-acting muscarinic antagonist (e.g., tiotropium, glycopyrronium, aclidinium, umeclidinium) for any reason, as an overdose may result. Clinically significant cardiovascular effects and fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs.
Anticholinergic Effects: Consistent with its antimuscarinic activity, TRELEGY ELLIPTA should be used with caution in patients with narrow-angle glaucoma (see Ophthalmologic as follows) or urinary retention (see Renal as follows) since worsening of these conditions may occur.
Cardiovascular: Cardiovascular effects, such as cardiac arrhythmias, e.g., atrial fibrillation and tachycardia, may be seen after the administration of sympathomimetic agents and muscarinic receptor antagonists, including TRELEGY ELLIPTA. In case such effects occur, treatment may need to be discontinued.
Clinically significant cardiovascular effects and fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs. Cardiovascular effects such as tachycardia, arrhythmia, palpitations, myocardial ischemia, angina pectoris, hypertension or hypotension have been associated with use of beta-adrenergic agonists. In addition, beta-agonists have been reported to produce electrocardiographic changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. Like all products containing sympathomimetic agents, TRELEGY ELLIPTA should therefore be used with caution in patients with unstable or life-threatening cardiovascular disease, especially coronary insufficiency, cardiac arrhythmias (including tachyarrhythmias), or hypertension.
Electrocardiography: As with other beta2-agonists, caution is recommended if TRELEGY ELLIPTA is administered to patients with a known history of QTc prolongation, risk factors for torsade de pointes (e.g., hypokalemia), or patients who are taking medications known to prolong the QTc interval (see Interactions and Pharmacology: Pharmacodynamics under Actions).
Hemodynamics: Like other beta2-agonists, vilanterol can produce clinically significant cardiovascular effects in some patients as measured by an increase in pulse rate, systolic or diastolic blood pressure, or cardiac arrhythmias such as atrial fibrillation, supraventricular tachycardia and extrasystoles (see Adverse Reactions and Pharmacology under Actions). If such effects occur, TRELEGY ELLIPTA may need to be discontinued.
Driving and Operating Machinery: There have been no studies investigating the effect of TRELEGY ELLIPTA on the ability to perform tasks that require judgment, motor or cognitive skills. The occurrence of headache or blurred vision may influence the ability to drive or to use machinery.
Ear/Nose/Throat: Localized infections of the mouth and pharynx with Candida albicans, which are associated with the use of inhaled glucocorticosteroids, have occurred in patients treated with TRELEGY ELLIPTA during clinical studies. Patients should therefore be advised to rinse their mouth with water (without swallowing) after inhalation of TRELEGY ELLIPTA to reduce the risk of oropharyngeal candidiasis.
When such an infection develops, it should be treated with appropriate local or systemic (i.e., oral) antifungal therapy while treatment with TRELEGY ELLIPTA continues. However, at times, therapy with TRELEGY ELLIPTA may need to be interrupted for the treatment of severe infections (see Interactions).
Endocrine and Metabolism: Systemic effects of inhaled corticosteroids may occur, particularly at high doses prescribed for prolonged periods. These effects are much less likely to occur with inhaled corticosteroids than with oral corticosteroids. Possible systemic effects include: Cushing's syndrome, Cushingoid features, hypothalamic-pituitary-adrenal (HPA) axis suppression, growth retardation in children and adolescents (in asthma), a decrease in bone mineral density (BMD), cataracts, glaucoma, and central serous chorioretinopathy.
Hypercorticism and Adrenal Suppression: Inhaled fluticasone furoate is absorbed into the circulation and can be systemically active (see Pharmacology: Pharmacodynamics under Actions). Exceeding the recommended dosage or co-administration with a strong cytochrome P450 3A4 (CYP3A4) inhibitor may result in HPA dysfunction (see Interactions).
It is possible that systemic corticosteroid effects such as hypercorticism and adrenal suppression (including adrenal crisis) may appear in a small number of patients who are sensitive to these effects. In light of the possibility of systemic absorption of inhaled corticosteroids, patients treated with TRELEGY ELLIPTA should be observed carefully for any evidence of systemic corticosteroid effects. Particular care should be taken in observing patients postoperatively or during periods of stress for evidence of inadequate adrenal response. If such effects occur, appropriate therapy should be considered.
Systemic Steroid Replacement by Inhaled Steroid: Particular care is needed for patients who have been transferred from systemically active corticosteroids to inhaled corticosteroids because deaths due to adrenal insufficiency have occurred in patients with asthma during and after transfer from systemic corticosteroids to less systemically available inhaled corticosteroids. After withdrawal from systemic corticosteroids, a number of months are required for recovery of HPA function.
Patients who have been previously maintained on 20 mg or more of prednisone (or its equivalent) may be most susceptible, particularly when their systemic corticosteroids have been almost completely withdrawn. During this period of HPA suppression, patients may exhibit signs and symptoms of adrenal insufficiency when exposed to trauma, surgery, or infection (particularly gastroenteritis) or other conditions associated with severe electrolyte loss. Although TRELEGY ELLIPTA may control COPD or asthma symptoms during these episodes, in recommended doses it supplies less than normal physiological amount of glucocorticoid systemically and does NOT provide the mineralocorticoid activity that is necessary for coping with these emergencies.
During periods of stress, a severe asthma attack, or a severe COPD exacerbation, patients who have been withdrawn from systemic corticosteroids should be instructed to resume oral corticosteroids immediately and to contact their physicians for further instruction. These patients should also be instructed to carry a warning card indicating that they may need supplementary systemic corticosteroids during periods of stress, a severe asthma attack, or severe COPD exacerbation.
Patients requiring oral corticosteroids should be weaned slowly from systemic corticosteroid use after transferring to TRELEGY ELLIPTA. Lung function (mean forced expiratory volume in 1 second [FEV1]), beta-agonist use, and COPD or asthma symptoms should be carefully monitored during withdrawal of oral corticosteroids. In addition, patients should be observed for signs and symptoms of adrenal insufficiency, such as fatigue, lassitude, weakness, nausea and vomiting, and hypotension.
Transfer of patients from systemic corticosteroid therapy to TRELEGY ELLIPTA may unmask allergic conditions previously suppressed by the systemic corticosteroid therapy (e.g., rhinitis, conjunctivitis, eczema, arthritis, eosinophilic conditions).
During withdrawal from oral corticosteroids, some patients may experience symptoms of systemically active corticosteroid withdrawal (e.g., joint and/or muscular pain, lassitude, depression), despite maintenance or even improvement of respiratory function.
Reduction in Bone Mineral Density: Decreases in bone mineral density (BMD) have been observed with long-term administration of products containing inhaled corticosteroids. Patients with major risk factors for decreased bone mineral content, such as prolonged immobilization, family history of osteoporosis, postmenopausal status, tobacco use, advanced age, poor nutrition, or chronic use of drugs that can reduce bone mass (e.g., anticonvulsants, oral corticosteroids) should be monitored and treated with established standards of care. Since patients with COPD often have multiple risk factors for reduced BMD, assessment of BMD is recommended prior to initiating TRELEGY ELLIPTA and periodically thereafter. If significant reductions in BMD are seen and TRELEGY ELLIPTA is still considered medically important for that patient's COPD therapy, use of medication to treat or prevent osteoporosis should be strongly considered.
Effect on Growth: Inhaled corticosteroids may cause a reduction in growth velocity when administered to children and adolescents (see Pharmacology: Pharmacokinetics under Actions).
Hypokalemia and Hyperglycemia: Beta-adrenergic agonist medications may produce significant hypokalemia in some patients, which has the potential to produce adverse cardiovascular effects. The decrease in serum potassium is usually transient, not requiring supplementation. TRELEGY ELLIPTA should be used with caution in patients predisposed to low levels of serum potassium. In patients with severe COPD, hypokalemia may be potentiated by hypoxia and concomitant treatment (see Interactions), which may increase the susceptibility to cardiac arrhythmias.
Beta-agonist medications may produce transient hyperglycemia in some patients.
Co-existing Conditions: TRELEGY ELLIPTA, like all medications containing sympathomimetic amines, should be used with caution in patients with convulsive disorders or thyrotoxicosis and in those who are unusually responsive to sympathomimetic amines. Doses of the rapid onset, short-duration, beta2-adrenoceptor agonist salbutamol, when administered intravenously, have been reported to aggravate pre-existing diabetes mellitus and ketoacidosis.
Hematologic: Eosinophilic Conditions: In rare cases, patients on inhaled corticosteroids may present with systemic eosinophilic conditions, with some patients presenting with clinical features of vasculitis consistent with eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as Churg-Strauss syndrome, a condition that is often treated with systemic corticosteroid therapy. These events usually, but not always, have been associated with the reduction and/or withdrawal of oral corticosteroid therapy following the introduction of inhaled corticosteroids. Physicians should be alerted to eosinophilia, vasculitic rash, worsening pulmonary symptoms, cardiac complications, and/or neuropathy presenting in their patients. A causal relationship between inhaled corticosteroids and these underlying conditions has not been established.
Hepatic/Biliary/Pancreatic: Hepatic Impairment: TRELEGY ELLIPTA has not been studied in patients with hepatic impairment (see Dosage & Administration). Information on the individual components is provided as follows.
Fluticasone Furoate/Vilanterol: Fluticasone furoate systemic exposure increased by up to 3-fold in subjects with mild, moderate and severe hepatic impairment. Patients should be monitored for corticosteroid-related systemic effects. For patients with moderate to severe hepatic impairment, the 100/62.5/25 mcg dose should be used (see Pharmacology: Pharmacokinetics under Actions). Hepatic impairment had no effect on vilanterol systemic exposure.
Umeclidinium: Subjects with moderate hepatic impairment (Child-Pugh score of 7-9) showed no relevant increase in systemic exposure to umeclidinium (Cmax and AUC), and no relevant difference in protein binding between subjects with moderate hepatic impairment and healthy volunteers. Umeclidinium has not been evaluated in subjects with severe hepatic impairment.
Hypersensitivity Reactions: Hypersensitivity reactions such as anaphylaxis, angioedema, rash, and urticaria may occur after administration of TRELEGY ELLIPTA. If signs suggesting allergic reactions (in particular, difficulties in breathing or swallowing, swelling of tongue, lips and face, urticaria, skin rash) occur, discontinue TRELEGY ELLIPTA. The patient should NOT be re-challenged with TRELEGY ELLIPTA if this is identified as the cause of the hypersensitivity reaction (see Contraindications).
There have been reports of anaphylactic reactions in patients with severe milk protein allergy after inhalation of other powder medications containing lactose; therefore, patients with severe milk protein allergy should not use TRELEGY ELLIPTA (see Contraindications).
Immune: Patients who are using drugs that suppress the immune system are more susceptible to infections than healthy individuals. Chickenpox and measles, for example, can have a more serious or even fatal course in susceptible patients using corticosteroids. In such patients who have not had these diseases or been properly immunized, particular care should be taken to avoid exposure. If a patient is exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) may be indicated. If a patient is exposed to measles, prophylaxis with pooled intramuscular immunoglobulin (IG) may be indicated. If chickenpox develops, treatment with antiviral agents may be considered.
It is important that even mild chest infections be treated immediately since COPD patients may be more susceptible to damaging lung infections than healthy individuals. Patients should be instructed to contact their physician as soon as possible if they suspect an infection.
Physicians should recommend that patients receive an annual influenza vaccination.
As with all medications containing a corticosteroid, TRELEGY ELLIPTA should be administered with caution, and only if necessary, in patients with active or quiescent tuberculosis infections of the respiratory tract; chronic or untreated infections such as systemic fungal, bacterial, viral, or parasitic; or ocular herpes simplex.
Monitoring and Laboratory Tests: Potentially serious hypokalemia has been observed with other beta-agonist therapies, which may increase susceptibility to cardiac arrhythmias. It is therefore recommended that serum potassium levels be monitored in patients predisposed to low levels of serum potassium.
Due to the hyperglycemic effect observed with other beta-agonists, additional blood glucose monitoring is recommended in diabetic patients.
For patients at risk, monitoring of bone and ocular effects (cataract, glaucoma, and central serous chorioretinopathy) should also be considered in patients receiving maintenance therapy with TRELEGY ELLIPTA.
Patients with hepatic impairment should be monitored for corticosteroid effects due to potentially increased systemic exposure of fluticasone furoate.
Ophthalmologic: Glaucoma and increased intraocular pressure have been reported in patients following the long-term administration of inhaled corticosteroids or with use of inhaled anticholinergics. Cataracts have also been reported in patients following the long-term administration of inhaled corticosteroids.
Long-term administration of inhaled corticosteroids may result in central serous chorioretinopathy (CSCR).
TRELEGY ELLIPTA, like other antimuscarinic-containing products, should be used with caution in patients with narrow-angle glaucoma. Prescribers and patients should also be alert for signs and symptoms of acute narrow-angle glaucoma (e.g., eye pain or discomfort, blurred vision, visual halos or colored images in association with red eyes from conjunctival congestion and corneal edema). Instruct patients to consult a healthcare professional immediately if any of these signs or symptoms develops.
Close monitoring is warranted in patients with a change in vision or with a history of increased intraocular pressure, narrow- or open-angle glaucoma, cataracts, and/or CSCR.
Renal: TRELEGY ELLIPTA, like other antimuscarinic-containing products, should be used with caution in patients with urinary retention. Prescribers and patients should be alert for signs and symptoms of urinary retention (e.g., difficulty passing urine, painful urination), especially in patients with prostatic hyperplasia or bladder-neck obstruction. Instruct patients to consult a healthcare professional immediately if any of these signs or symptoms develops.
Respiratory: Paradoxical Bronchospasm: As with other inhalation therapies, paradoxical bronchospasm may occur with an immediate increase in wheezing after dosing, and may be life-threatening. This should be treated immediately with a rapid onset, short duration inhaled bronchodilator such as salbutamol. Treatment with TRELEGY ELLIPTA should be discontinued immediately, the patient assessed and alternative therapy instituted if necessary.
Pneumonia: COPD: In line with the known class effect of inhaled corticosteroids, pneumonia events (including pneumonias resulting in hospitalization) were observed in patients with COPD receiving TRELEGY ELLIPTA. In some instances, fatal events of pneumonia have been reported with use of inhaled corticosteroid fluticasone furoate-containing drugs, including TRELEGY ELLIPTA (see Adverse Reactions). Physicians should remain vigilant for the possible development of pneumonia in patients with COPD, as the clinical features of such infections overlap with the symptoms of COPD exacerbations. Risk factors for pneumonia in patients with COPD receiving inhaled corticosteroid-containing drugs include current smokers, patients with a history of prior pneumonia, patients with low body mass index and patients with severe COPD. These factors should be considered when TRELEGY ELLIPTA is prescribed, and treatment should be re-evaluated if pneumonia occurs.
There is no conclusive clinical evidence for intra-class differences in the magnitude of the pneumonia risk among inhaled corticosteroid products.
Asthma: An increased incidence of pneumonia in patients with asthma receiving higher doses of TRELEGY ELLIPTA cannot be excluded. This is based on clinical experience with fluticasone furoate/vilanterol, where there was a trend toward an increased risk of pneumonia for fluticasone furoate/vilanterol 200/25 mcg compared with fluticasone furoate/vilanterol 100/25 mcg and placebo.
Use in children: Pediatrics (<18 years of age): TRELEGY ELLIPTA is not indicated for use in children and therefore should not be used in patients under 18 years of age (see Dosage & Administration).
Use in the elderly: Geriatrics (≥65 years of age): Based on the available data, there is no need to adjust the dose in elderly patients, but greater sensitivity of some older individuals cannot be ruled out (see Dosage & Administration).